The state of the older people’s healthcare workforce: A report from the BGS membership survey
This report summarises the findings of a survey of the BGS membership undertaken in the second half of 2023. It provides a snapshot into how our members are feeling about their work and the services they work in.

Foreword
We last surveyed the BGS membership in the midst of the COVID-19 pandemic. The survey was designed to gather intelligence specifically about our members’ experiences during the pandemic – the challenges they faced and how the services they worked in were meeting these challenges. While COVID is very much still present in our healthcare systems, the emergency posed by the virus has passed. We are aware, however, that the situation faced by our members daily is still incredibly tough.
Healthcare professionals should receive fair pay for the crucial work that they do but they are generally not motivated by money."
|
Professor Adam Gordon |
Dr Amit Arora |
|
BGS President |
BGS Vice President for Workforce |

Introduction
During summer and autumn 2023, the British Geriatrics Society (BGS) surveyed members via SurveyMonkey. Our aim in doing this was twofold. Firstly, we wanted to gather workforce information from across our multidisciplinary membership. We knew that through the annual census conducted by the Royal College of Physicians1 we had access to rich quantitative data about our physician members. We understand from this census how many geriatricians there are across the country, where they are and some information about how they feel about their work. This is useful data and we used this in our Case for More Geriatricians2 report. However, we do not have equivalent data for our multidisciplinary members and this survey was, in part, an attempt to gather some of this data.
Our second reason for surveying the membership was to understand more about what is happening in their services around the country. While we will not claim that this survey gave us as much data on the multidisciplinary team as we were hoping for, it did give us an insight into how our members are feeling about the services they work in and the care they are currently providing for their patients.
The survey was open from 31 July 2023 until 9 October 2023 and was promoted to members through email and posts on X (formerly Twitter). At the time of the survey, BGS had 4,600 members across the multidisciplinary team; 359 people responded to the survey, representing around 8% of the total membership.
We regularly analyse data from the RCP census from the perspective of geriatric medicine and publish this analysis.3 Our latest analysis of the RCP data will be published shortly after this report is published. We have cross-referenced some of the findings from the census into this report where relevant.
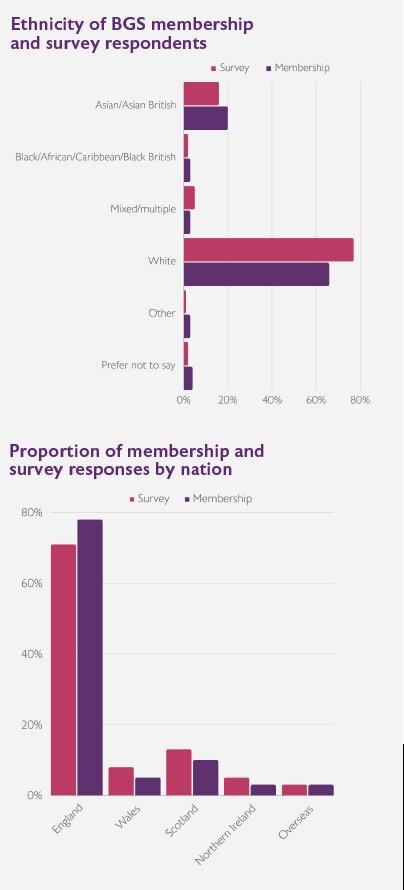
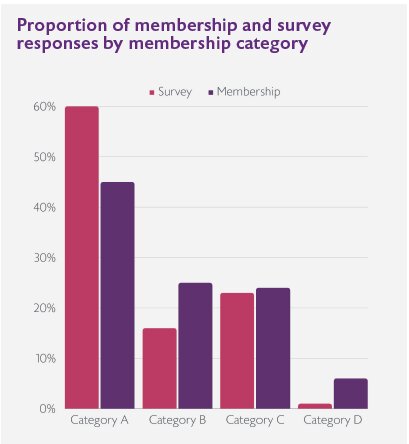
Who responded
Demographics
Work
i. Certificate of Completion of Training
ii. Certificate of Eligibility for Specialist Registration via the Combined Programme
iii. Membership data correct as of 31 December 2023.
iv. We were advised by members of our Trainees Council to use this terminology instead of ‘junior doctors’.

Results and analysis
To read the results and analysis of the survey, including direct quotes supplied by members and a call to action from BGS, please download the PDF of the report here.