Dr Jackie Martin-Kerry is a Research Fellow in Qualitative Process Evaluation at the University of Leicester. She is an applied health services researcher with interests in methodological development and frameworks. She tweets @JMartinKerry
Our research, published in Age and Ageing, reports which outcomes are most important to measure in hospital deprescribing trials with older people who are under the care of a geriatrician. Older people and their informal carers, health professionals and deprescribing researchers told us that six outcomes were most important, feasible and acceptable to collect and measure in hospital deprescribing research trials.
The development and importance of a Core Outcome Set
CHARMER (CompreHensive geriAtRician-led MEdication Review) is an NIHR-funded Ageing programme of research that aims to develop and test a hospital deprescribing intervention. In order for us to test the intervention in a research trial, we need to know which outcomes to measure. We developed a Core Outcome Set for hospital deprescribing trials for older people under the care of a geriatrician. A Core Outcome Set is a set of agreed outcomes that should be measured and reported, as a minimum, in all clinical trials testing an intervention for a particular health condition or area of healthcare. Trials can choose to collect other outcomes in addition to the Core Outcome Set to suit their context or focus. However, when all hospital deprescribing trials for older people under the care of a geriatrician collect and report the outcomes in this Core Outcome Set, results from similar trials can be compared and aggregated to develop an evidence base.
What were the challenges?
Despite following Core Outcome Set development guidance from the COMET (Core Outcome Measures in Effectiveness Trials), there were a number of methodological decisions to make. This included deciding on which method to use to incorporate the voices of stakeholders, with options including interviews, focus groups, nominal group technique, workshops and Delphi surveys.
We wanted to meaningfully engage older people and their informal carers in the process of developing our Core Outcome Set and so we used a Delphi survey, which is the most common method. We also had to choose a scale for stakeholders to rate the importance of each outcome; we chose the most commonly used 9-point scale. However, we found asking people to rate a long list of outcomes in terms of importance with this rating scale was burdensome on participants. We also found that asking people to rate the importance of outcomes using the scale did not give us a clear picture of which outcomes felt important However, having a Core Outcome Set with so many outcomes makes it less feasible for every trial to be able to measure all the outcomes in a Core Outcome Set. We found the planned subsequent workshops much more useful for stakeholders to discuss the outcomes and identify which ones were most important, or core, to include in the Core Outcome Set.
Usual practice is to finalise a Core Outcome Set and then later consider how to feasibly measure the outcomes, although not all Core Outcome Set studies think about how to measure the outcomes in their Core Outcome Set, and many do not make this information available. A Core Outcome Set may be ‘not fit for purpose’ if, for example, some of the outcomes cannot be measured, or are deemed too expensive or not acceptable to collect. Often patients and the public are not involved in this later decision process about measurement. We considered issues of measurement of the outcomes before finalising the Core Outcome Set and believe this will make it easier for deprescribing trials to collect and report these outcomes.
Which outcomes were included?
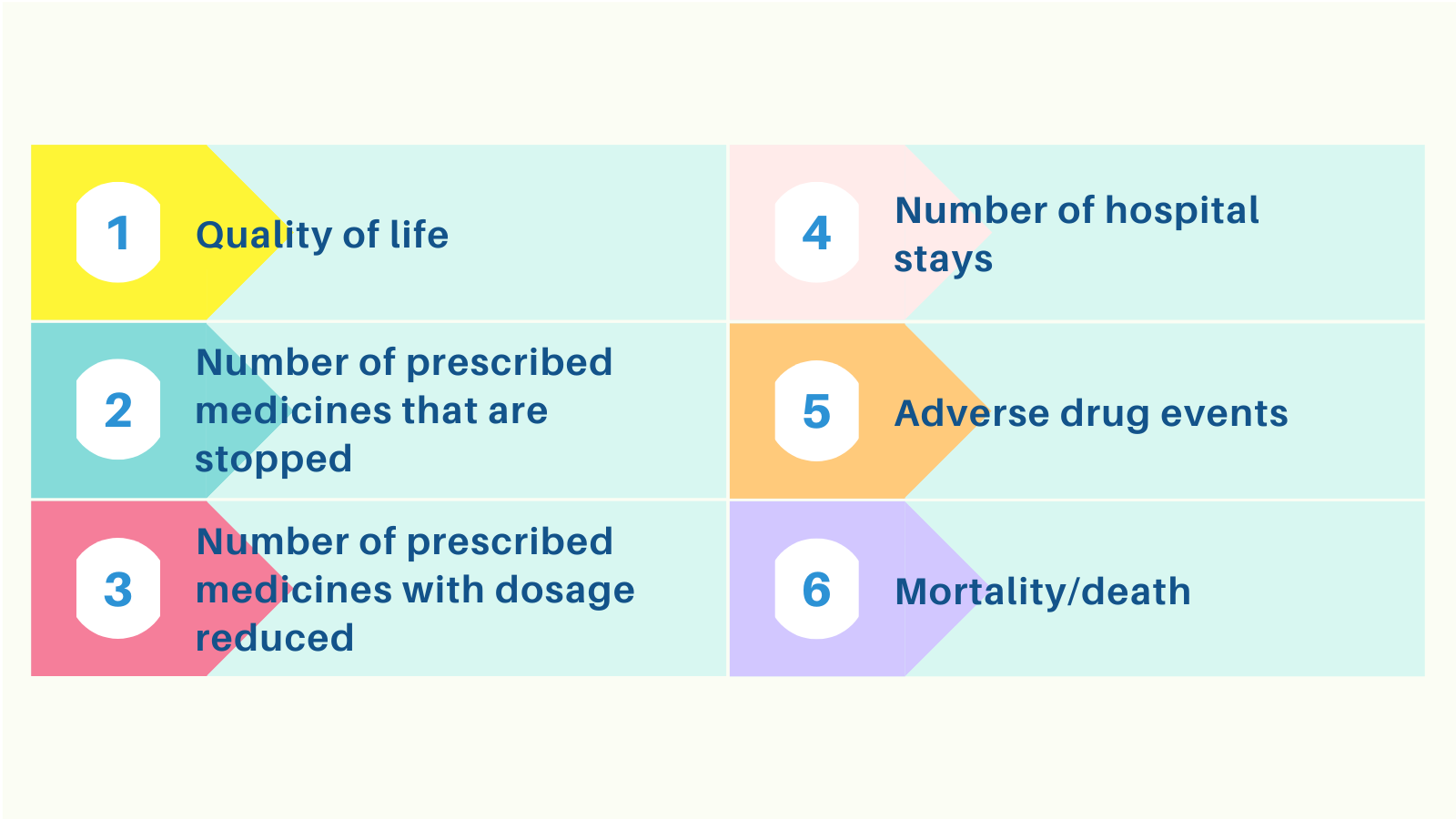
The six outcomes that were considered important and feasible to measure and are therefore included in the Core Outcome Set are: number of prescribed medicines stopped; number of prescribed medicines with dosage reduced; quality of life; mortality; adverse drug events; and number of hospital stays. Three outcomes were not included because they were deemed not feasible or acceptable to collect.
Future research
All hospital deprescribing trials for older people under the care of a geriatrician should adopt this Core Outcome Set and measure and report these outcomes. Further research is needed to identify how to best engage participants in the Core Outcome Set development process and how to incorporate measurement within the process to ensure the development of Core Outcome Sets that are ‘fit for purpose’ and subsequently used by relevant trials.
Read the full paper here on the Age and Ageing website: Developing a core outcome set for hospital deprescribing trials for older people under the care of a geriatrician