
Dr Pippa Collins is an advanced clinical practitioner and clinical academic working in the community in Bournemouth and Christchurch, Dorset. She has worked in acute hospitals in both the UK and USA before moving to her role in the community. She currently works in an advanced practice team which runs a hospital at home and is integrated with the Intermediate care team where they support people with frailty who have become acutely unwell.
The generalist workforce supports many people with frailty to die at home – are we doing this well? Having searched the research literature, I could find very little detail around how older people die with frailty at home. The literature that I did find was acute hospital centric and looked at metrics such as acute hospital admissions and emergency bed use. I wanted to understand what was happening in my community work in Dorset.
I included 50 people who were over 75, were mainly housebound, had no definitive terminal diagnosis and lived at home. I excluded 45 people who had a clear diagnosis of a terminal condition, those who lived in a care home or where specialist palliative services were involved. I included notes from GPs, 999, 111, community teams, acute and community hospitals.
The notes were reviewed to understand whether there was a crisis situation as the person died. I subjectively defined a crisis as an admission or emergency department (ED) visit in the last days of life, uncertainty and anxiety of the patient or supporters, poorly controlled symptoms, distressed relatives or care or equipment issues. Deaths that were anticipated and prepared for where appropriate equipment and support were in place. Symptoms were controlled and uncertainty minimised were classed as non-crisis. Some ‘non-crisis’ people may have had an appropriate urgent admission towards the time of their death, for example for an x-ray to inform pain management strategies.
I found that 23/50 people died in crisis as defined above, 10 of these in hospital. The main themes were a person’s wishes not being respected and supported, not being treated as end of life until actively dying causing crisis medical interventions, different perspectives from different healthcare professionals (HCPs), family not aware or accepting that the person was dying, poor health literacy of the person or supporter, rapidly escalating care needs not being met, no clinician taking clear ownership, a medical approach raising hope or expectation and poor symptom control, especially of agitation.
For the 27/50 people who did not die in crisis the overwhelming theme was that the person or supporter was strongly able to advocate for themselves enabling them to direct healthcare professionals to a supportive rather than a medical/crisis driven approach. Other themes were clear communication about dying from healthcare professionals over time, trigger events recognised and leading to a plan, family all on board and understanding, admission not repeatedly discussed, adequate equipment and support and good management of agitation.
Nineteen people had an advance care plan and 58% did not die in crisis; 52% of the 31 people without an advance plan did not die in crisis, suggesting that in our community the presence of an advance care plan had little effect on whether a crisis was avoided or not. This is perhaps because helping a person and their supporters to understand that the process of dying has started is complex, we are not taught these skills, healthcare professionals and, importantly, social carers lack confidence and there is a reliance on a medical model of crisis management.
From my findings, I developed a multi-stepped process (Fig. 1) which is informing the next stage of this quality improvement (QI) project.
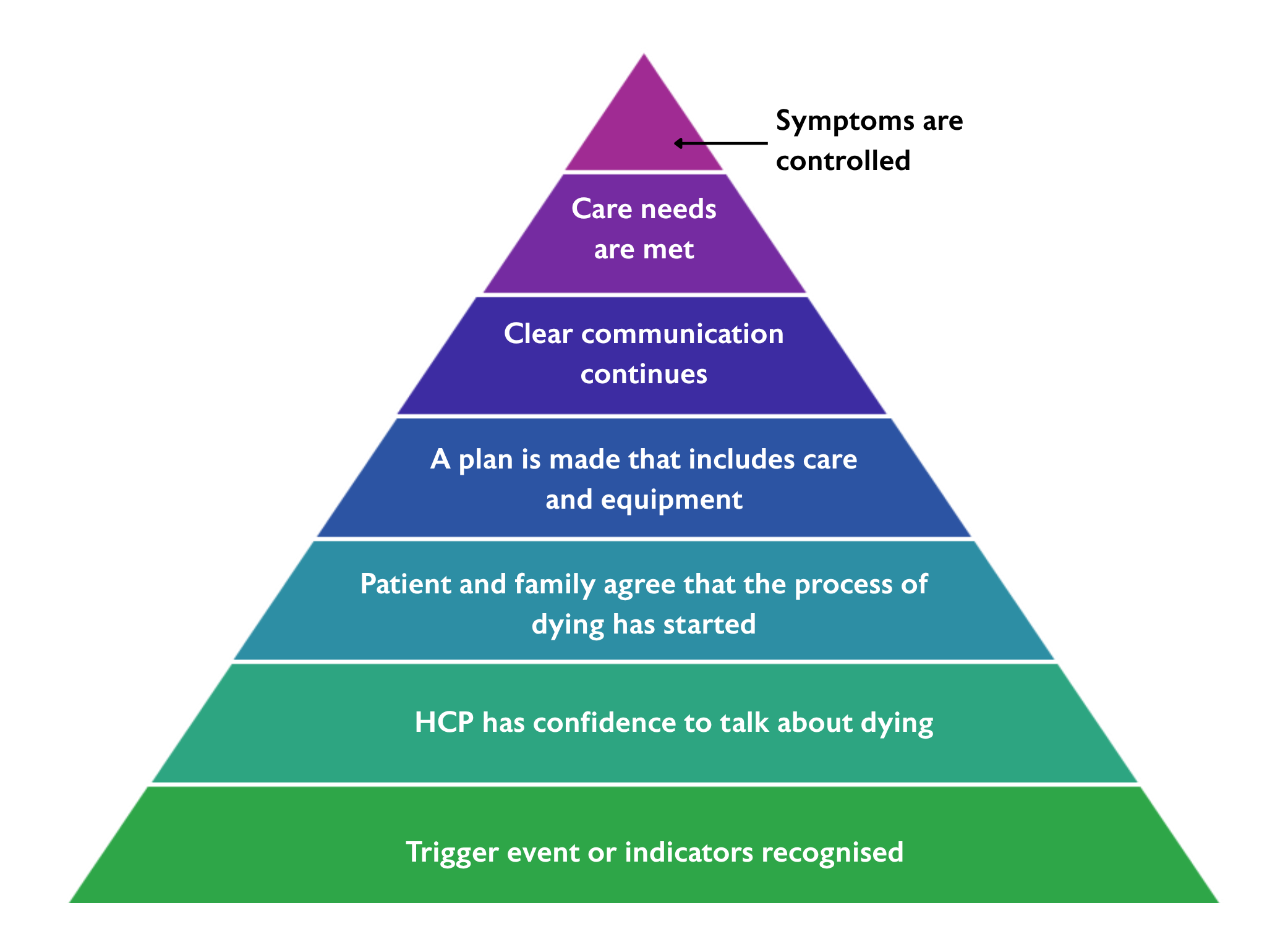
Figure 1: Multi-process informing the next stage of Pippa's QI project
Firstly, healthcare professionals who work with people with frailty need to recognise and act on trigger events or indicators using tools such as End of Life Care in Frailty: Identification and prognostication guide.
Next, we need to be able to confidently talk to patients and their supporters about these prognostic indicators and help them to navigate the uncertainty inherent in the dying frailty trajectory. If the patient and supporters agree that the process of dying has started then a plan can be made, and a crisis avoided. Without full understanding and agreement at this point, the advance plan is at risk of being overruled with crisis driven rather than supportive and symptomatic care implemented.
Plans must include social support. People dying of frailty frequently have high care needs that escalate rapidly towards the end. Without skilled, responsive care that is available at night, people cannot be supported to die well with frailty. Additionally, the main symptom at end of life in this QI project was terminal agitation, often interpreted as 'a UTI' and as such poorly managed. Interestingly, evening and night time agitation or disorientation appeared as a precursor to dying in a number of people several weeks prior to death.
This preliminary work has led to the development of a working group who are now developing an exemplar team to implement the model in Fig 1. We are also planning a qualitative exploration of the experiences and understandings of patients and supporters as they navigate the final stages of severe frailty.


