Introduction
Training Programme Directors (TPDs) hold a unique system-wide perspective on the structure, delivery and challenges of geriatric medicine higher specialty training. They are well placed to understand the factors influencing recruitment, retention, progression and training quality.
The TPD survey has been a valuable tool for the BGS to gain insight into variations in working patterns and training provision, as well as help to identify common challenges. The survey has been conducted across multiple iterations, including in 2016, 2019 and 2023, enabling analysis of trends over time. By combining these insights with existing national data, this report seeks to inform future workforce planning and support the development of a sustainable pipeline of geriatricians for the future.
About
TPDs across the UK were invited by the BGS to complete an electronic survey via email. The survey this year was streamlined to 28 questions, focusing predominantly on training patterns and workforce metrics, with an additional subset addressing training opportunities within community geriatrics.
The survey was open for six weeks in Autumn 2025, aligning with the start of the academic training year across all deaneries. Seventeen completed responses were received initially, with one further response received when the survey was reopened for a second time in December. Data was captured from the following deaneries: London North Central and East, London South East, Thames Valley, Yorkshire, Scotland (North), Scotland (West), Scotland (South East), Wales, East of England, East Midlands (North), Severn, Kent, Surrey and Sussex, Wessex and Peninsula.
Results and reflections
National Training Numbers and Vacancies
National Training Numbers (NTNs) are a unique identifier assigned to doctors in UK specialty training programs (such as geriatric medicine) that lead to a Certificate of Completion of Training (CCT).
Of the reported 517 NTNs in geriatric medicine across the UK, 37 places were reported to be unfilled, suggesting a vacancy rate of 7.2%. This is comparable to rates observed in previous TPD surveys (6.8% in 2023, 7.6% in 2019 and 6.9% in 2016).
NHS England Medical Specialty Recruitment data demonstrates that applications to geriatric medicine have increased in recent years (266 applicants for 148 posts in 2023; 281 for 161 in 2024; and 323 for 157 in 2025). However, this rise appears to reflect a broader system-wide trend rather than growth specific to the specialty.
Increases in competition have been uneven across specialties. Surgical training, radiology, and psychiatry have experienced disproportionately larger rises, whereas others, such as geriatric medicine and acute internal medicine, have continued to demonstrate comparatively lower competition ratios and persistently underfilled posts.
With fill rates of approximately 83% in 2023, 73% in 2024, and 80% in 2025, geriatric medicine has remained an under-recruited speciality. This is despite the national picture of increasing competition and demand for spaces. This divergence between increasing application numbers and ongoing under-recruitment suggests that application volume does not directly translate into successful appointments. Contributing factors likely include multiple applications per candidate, preferential ranking of alternative specialties, and geographical variation in post uptake.
While not all TPDs could provide data on Locum Appointment for Training/Locum Appointment for Service (LAT/LAS) posts, a minimum of 28 posts were identified. This indicates a substantial workforce contribution. This analysis does not account for the contribution of those progressing through alternative routes to consultant practice such as Specialty and Associate Specialist (SAS) doctors or those progressing via the Portfolio Pathway (previously known as Certificate of Eligibility for Specialist Registration - CESR), who represent an important component of the wider workforce.
Less Than Full Time Training
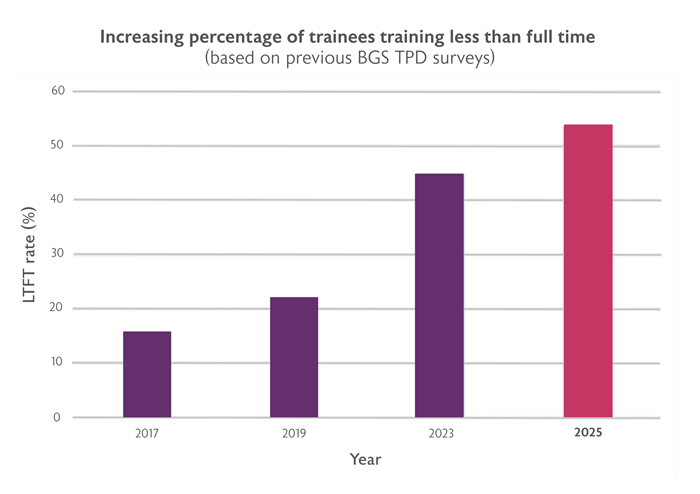
The TPD survey demonstrates that 53.6% of NTN trainees work less than full time (LTFT). Most TPDs reported that over 50% of the trainees in their deanery were working less than full time. This proportion has been steadily growing in recent years. 44.8% of trainees were reported to be working on a LTFT basis in 2023, 22% in 2019 and 15.8% in 2017. At least 61 trainees entered LTFT from ST4. Most trainees apply for LTFT under category 1 but there are an increasing number who apply under category 3 (see table below).
| Region | LTFT | Cat 1 | Cat 2 | Cat 3 | LTFT rate |
| England | 214 | 154 | 9 | 51 | 52.6% |
| Scotland | 37 | 29 | 4 | 4 | 59.6% |
| Wales | 26 | 4 | 0 | 22 | 54.2% |
Cat 1: Health reasons or responsibility towards dependents
Cat 2: Unique opportunities
Cat 3: Personal choice
Several deaneries additionally reported trainees commencing ST4 training on LTFT arrangements. Among deaneries able to provide data, a median of 50% of trainees entered ST4 training LTFT (range 12.5%–100%), suggesting that flexible training is increasingly being incorporated from the point of entry into higher specialty training.
The BGS is supportive of initiatives that enable clinicians to work LTFT or in other flexible arrangements. We have recently updated our position statement on this issue.
Time Out of Programme (OOP)
At least 41 trainees were reported to be on an OOP experience at the time of the survey. Common areas were in stroke, research and leadership. We did not specifically explore the number of trainees undertaking integrated work schedules to facilitate personal development opportunities; however, a proportion of these individuals may be represented within the LTFT cohort, particularly under Category 2.
| Region | Stroke | Leadership | Research | Community | Other* | Total |
| England | 7 | 6 | 8 | 1 | 8 | 26 |
| Scotland | 3 | 2 | 2 | - | - | 7 |
| Wales | 1 | - | - | - | 1 | 2 |
| 11 | 8 | 10 | 1 | 32 |
*Other includes perioperative medicine, orthogeriatrics, onco-geriatrics and movement disorders
Completion of training
At least 77 trainees achieved their Certificate of Completion of Training (CCT) in the last year. Most trainees take up consultant roles locally (71 out of 77, 92%). The TPDs who responded to the survey are unaware of any trainees who achieved CCT who did not go on to take a consultant post.
Attrition
Five trainees were reported to currently be on long-term sick leave. At least four trainees left the rotation without CCT or CESR in the last year. One moved to a different specialty, one received outcome 4 (release from training with or without competencies) in Annual Review of Competence Progression (ARCP), one had to leave the country for personal reasons and one did not complete the geriatric Specialty Certificate Examination (SCE) and therefore only received CCT in general internal medicine (GIM),
Community rotations
14 deaneries confirmed that there are allocated community rotations for trainees (about 80%), However, there is variability in access and structure. The majority describe a mixture of experiences in Hospital at Home, domiciliary visits, community hospitals, and involvement in Primary Care Network (PCN) multidisciplinary team (MDT) discussions. One has commented that a trainee may not have a dedicated community rotation but felt that they are able to meet all the curriculum requirements within the four year rotation between the training sites.
Perceived Challenges of the TPD Role
Survey respondents described the role of the TPD as increasingly complex, with a central challenge being the need to balance training requirements with service pressures. The majority highlighted the difficulty of aligning trainees’ educational needs, preferences, and curriculum requirements with the operational demands of individual sites. This was compounded by limited staffing levels, with TPDs often required to prioritise service provision while striving to maintain the quality and breadth of training opportunities.
Workforce pressures were a prominent theme across responses. Several TPDs reported a high number of trainees approaching CCT within short timeframes, creating anticipated workforce gaps. This was further exacerbated by the widespread uptake of LTFT training, resulting in a significant reduction in whole-time equivalent (WTE) workforce capacity. Recruitment challenges, particularly in geographically large or less well-served regions, with downstream implications for both trainee distribution and the consultant workforce remain a recurring problem.
Administrative burden was also identified as a major constraint. Respondents described substantial workloads related to rotation planning, ARCP processes, and managing trainees on non-standard or out-of-sync pathways. This workload has increased in the context of diminishing deanery administrative support, including reduced assistance with ARCP coordination. Many TPDs noted that the time allocated within their job plans was insufficient to meet these demands. One highlighted perceived disparities in remuneration and programmed activities compared to other specialties.
A few respondents also emphasised challenges related to trainee support and progression. This included managing trainees who were experiencing difficulties and ensuring that trainees are adequately prepared for the transition to consultant roles. One felt the reduced continuity on wards also impacted supervision, teaching, and assessment. Supporting international medical graduates (IMGs), particularly at the start of training, was identified as requiring additional time and resources.
Finally, broader issues relating to the training environment were identified. These included variable engagement from consultant trainers, difficulties in promoting academic development among trainees, and challenges in expanding training opportunities, particularly within community settings, due to financial constraints and service pressures. Collectively, these findings highlight the multifaceted and evolving nature of the TPD role, shaped by competing demands across education, workforce, and service delivery.
Discussion
The findings from this survey provide an updated overview of the trainee population and the structure of geriatric medicine training across the UK, and highlight several consistent themes when compared with previous iterations of the TPD survey.
Overall, vacancy rates have remained relatively stable over time, suggesting that while geriatric medicine continues to experience challenges with recruitment, these have not significantly worsened in recent years. However, this stability should be interpreted cautiously, as it may mask regional variation and ongoing difficulties in filling posts in certain deaneries. In response to these challenges, the BGS launched the #ChooseGeriatrics campaign last year. During the first year, BGS shared 19 stories from individuals about why they chose to specialise in geriatrics and the #ChooseGeriatrics page has been viewed 2,012 times by 1,292 unique users. The Trainees Council has also introduced dedicated medical student representatives and expanded its support for Geriatric Medicine student societies across the UK.
Within the Foundation Programme and Internal Medicine Training (IMT) curriculum, most trainees will undertake a rotation in geriatric medicine, most commonly in an inpatient ward setting. These placements represent a valuable opportunity for the wider multidisciplinary team and consultant body to shape perceptions of the specialty, actively engage trainees, and promote the breadth of geriatric medicine.
As highlighted in our previous TPD Survey 2023 report, increasing competition for entry into IMT is likely to represent a major bottleneck in the training pathway to becoming a geriatrician. However, there appears to be strong retention once trainees enter specialty training, with many remaining within the same region after achieving CCT.
A key finding from this survey is the increasing prevalence of LTFT training and OOP experiences amongst trainees. The majority of deaneries reported that over half of their trainees are now training LTFT, alongside a notable number undertaking OOPE for research, leadership or other development opportunities. While this reflects a positive shift towards flexible and portfolio careers, it has important implications for workforce planning, rota design and training capacity. There is a widening mismatch between workforce flexibility and training system capacity, which TPDs have identified as one of the most significant challenges they face.
Addressing these issues will require a more coordinated approach to workforce and training design, including models that move beyond simple headcount and better reflect whole-time equivalent staffing. The development of more flexible and resilient rota structures will be important in mitigating gaps, particularly in the context of ongoing service pressures. This includes greater standardisation of flexible working approaches, including job sharing where feasible, as explored in the previous TPD 2023 survey report. Supporting TPDs and organisations to implement these approaches effectively will be essential. In line with this, the BGS has recently updated our position statement on flexible working which includes practical guidance to support rota design.
As the field of geriatric medicine continues to evolve, it is important that training programmes evolve alongside it. With the increasing shift in care delivery from hospital to community settings, we recognise the need for future geriatric consultants to receive adequate training and exposure in community geriatrics. From the results of this survey, there appears to be substantial regional variability in community geriatrics exposure. Training experiences involving home visits and virtual wards may offer particularly valuable insight into evolving models of community-based care compared to the community hospital placements which more closely resemble conventional inpatient practice. In addition, the duration and extent of community geriatrics exposure for individual trainees remains unclear. A recent survey conducted by the BGS Community Geriatrics Special Interest Group exploring trainees’ experiences in community geriatrics will hopefully provide valuable additional insight in this area.
A small number of TPDs also raised concerns regarding preparedness for transition to consultant practice. While numbers were too low to draw firm conclusions, this may reflect wider challenges associated with increasing service pressures, alongside the need to ensure sufficient exposure to leadership, managerial responsibilities, and independent decision-making during training. Training programmes should aim to adequately prepare trainees for consultant practice by providing opportunities for broader leadership and management experience beyond rota coordination or teaching organisation. Some trainees are also seeking additional development in these areas through OOPE opportunities. The BGS hopes to support this transition by enhancing its leadership programmes.
Limitations
This survey has several limitations. Response rates were incomplete, with data unavailable from a number of deaneries, which may limit the generalisability of the findings. In addition, responses relied on TPD-reported data, which may be subject to variation in interpretation.
Interpretation of the findings, particularly the quantitative data, should be undertaken with caution given the incomplete national representation. This was further compounded by potential ambiguity in questions relating to NTNs, which may have resulted in variable interpretation and reporting across TPDs. In particular, there was variability in the interpretation of ‘NTNs allocated’, with some respondents reporting annual recruitment numbers or current trainee headcount rather than total training capacity. Future surveys would benefit from clearer wording and additional clarification within the survey to improve consistency of reporting.
Recommendations and next steps
- Organisations such as the BGS may wish to consider publishing “Best practice” examples to show how trainee doctors can be given varied experiences, such as community-based posts, during their training
- Trusts should increase allocated programmed activities for TPD roles in recognition of the changing nature and demands of this role.
- Bodies responsible for medical training across the UK should improve national data capture on trainee pathways
- Bodies responsible for medical training across the UK should commit strategic investment in training infrastructure and leadership support is required to ensure sustainability.


