Dr Lara Mitchell is a Consultant Geriatrician at Queen Elizabeth University Hospital (QEUH), Glasgow. She is clinical lead for acute and has developed a frailty service. She is Chair of the BGS Cardiovascular SIG and tweets @laramitchdr
As we waited for COVID-19 to hit us, I felt an incredible sense of urgency on both an individual and societal level, that we would have to talk about dying during this pandemic. We can easily concentrate on the numbers of deaths, but the narrative behind the numbers, and what this means for those individuals and families, is also important. At medical school we are taught all about lifesaving treatments and how to treat any ailment a patient might have. Yet I think we still struggle with the concept that caring for the dying and providing a good death are equally as important as cure.
Last week I visited one of my patients, with suspected COVID-19. She was in a single room and I wore full PPE. I talked with her, using my eyes to convey empathy. We filled out her ‘what matters to me’ board, behind her bed, listing her favourite TV programme, her tea with lots of milk, her new grandchild and her family. I said to her ‘I am going to phone your family- what would you like me to tell them?’ She replied, ‘Tell them that I love them.’
I have been a Consultant for 17 years but this kind of social isolation for patients, with staff in PPE and family unable to visit, is a new and distressing challenge for me. I wrote up her case notes with tears in my eyes, and it really struck home that hard as this of course is for patients themselves, it is also really tough for everyone.
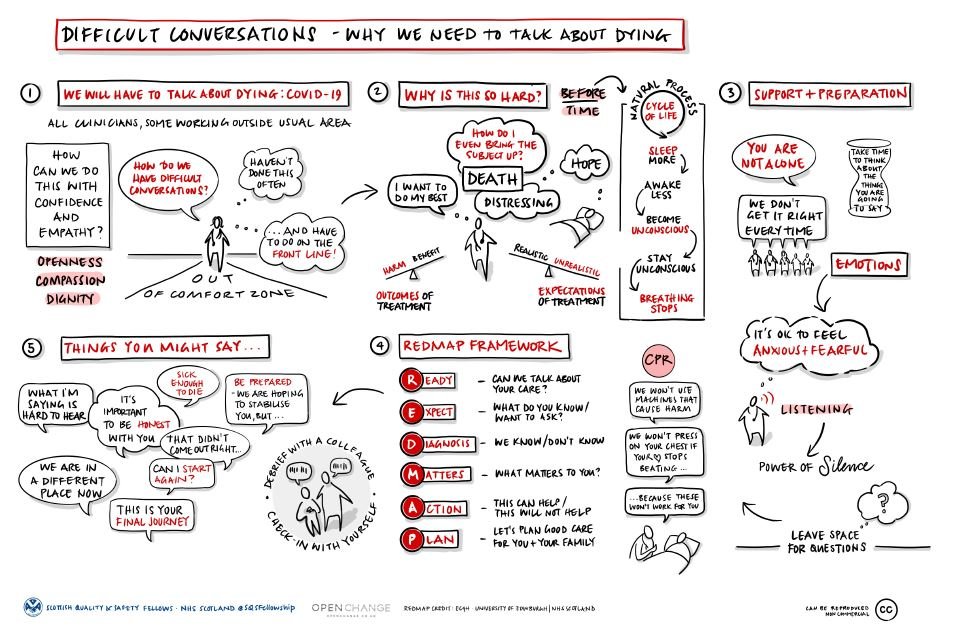
We must talk about dying during COVID-19, but the challenge for us is how to do this with confidence and empathy and have these conversations with openness, compassion and dignity. For many of us we may feel out of our comfort zone. This is really hard and death is distressing. We want to do our best, give the patient hope, and have our own hopes for them. In our minds, we weigh up the outcomes of treatment, what may cause harm and what will cause benefit, and try to match this with the patient’s expectation of treatment. This includes considering early decisions around CPR, when patients present to the hospital.
We all have to face death - it’s a natural process in the cycle of life. Unfortunately, for some people this natural process will be before their anticipated time. Understanding the process of dying helps us explain it clearly and simply to our relatives and patients. We know that people sleep more, are awake less, become unconscious for periods of time, then stay unconscious, and finally stop breathing. However, everyone has a different journey through this process which can make it hard to fully predict.
We need to prepare ourselves for these conversations and also acknowledge the emotion within them. It’s ok to feel anxious and fearful about broaching these issues, and regardless of experience, we do not get it right every time. We need to absolutely listen to our patients, to use that power of silence, and leave space for their questions. Silences over the phone are hard - there are natural ones and then longer ones, so having a feel of when to check in with the person on the other end, is important.
The ‘REDMAP’ framework (thanks to colleagues in Edinburgh) can help these conversations:
- Ready: Have you put the job-list down, and are you in a space where you are ready to do this? If talking with relatives, check where they are, if someone is with them and verify if they are happy to proceed. If it's the patient, ask “Can we talk about your care?”
- Expect: Check their understanding – are you on the same page, or do you have more explaining to do? For example ask “what do you know so far?” or ’’what do you want to ask?”.
- Diagnosis: Explain what we know and don’t know. Be open and honest
- Matters: What matters to them? It may be to see a certain member of family / their dog, or something else altogether. Ask. Listen.
- Action: Use clear language to let them know what can help, and what will not help.
- Plan: Make a plan so everyone knows what to do and document this clearly in the notes.
Over my time having these conversations I have built my own language about how I communicate to patients and families. It’s helpful to have some phrases that you can use and are confident in using. Mine have developed over time and are based on experience and my observations of incredible colleagues in the UK.
Some that I use are:
“What I am saying is hard to hear”, “we are in a different place now”, “it is important to be honest with you”, “be prepared that we are hoping to stabilise you” and sometimes, “that didn’t come out right, can I start again?” We should make families aware that their loved one is sick enough to die, that we are concerned about them, and that this may be their final journey.
Many of us are going to be doing this over the next few months and it is also really important that you are able to debrief with a colleague and check-in with yourself about how you are. My colleague and I do this regularly, and it helps to share the experience.
We are in this together and must never forget that. We also need to have these conversations with our patients - and ensure they are open, honest and compassionate.