
Disaster medicine involving older people
Disasters can be triggered by natural catastrophes such as blizzards, hurricanes, earthquakes, tsunamis, tornados, heat waves, fires, and floods, as well as human borne tragedies such as mass shootings, industrial accidents, and chemical, biological, nuclear and explosive events.
Disaster management in relation to frail, older populations has historically focused upon pre-planning preparations and post-disaster evacuation from harm and provision of shelter and nutrition. Disasters such as Hurricane Katrina in 2005 demonstrated that frail older people experience a disproportionate number of deaths. These suboptimal outcomes are associated with older adults’ age-related comorbidities and reduced mobility, in conjunction with system-level barriers to emergency evacuation and reduced access to timely medical management and prescription medications following a disaster. Consequently, the American Red Cross and American Academy of Nursing published recommendations to improve patient- and system-level preparedness.275
|
Patient/caregiver recommendations |
|
|
Community recommendations |
|
|
Healthcare recommendations |
|
|
Hospital/nursing home recommendations |
|
Older adults and their caregivers are often unprepared for the chaos following a disaster, whether they reside in North America,276 Asia,277 or Australia.278 This gap is apparent across socioeconomic subgroups276 and paradoxically accentuated among dementia caregivers.277 Even long-term care facilities exhibit gaps in preparedness to accommodate dementia patients during disasters.279 Older adults also report fewer social ties and less financial resource during disasters.280The likelihood of becoming homebound following a disaster is associated with the distance from the home to the closest retail stores.281
A particularly vulnerable subset of older adults are nursing home residents, who have worse morbidity and mortality when evacuated from their facilities,282 and these facilities are often not adequately prepared to maintain patient care while simultaneously confronting hazards such as power outages from natural disasters.283 Coordination of community resources when planning for disasters in older individuals should incorporate both nursing home and assisted living facility populations, as well as ventilator and dialysis dependent patients.284
Frail older patients are at higher risk for poor outcomes following intentional events because they are more likely to have a lower threshold of dangerous exposure to chemical and nuclear events, and be at higher risk of infection from biological events. They may not have typical presentations in relation to toxidromes (see section on non-specific presentations) and have increased trauma risk following explosions and penetrating injuries (see section on trauma).285 Standard approaches to managing patients after large-scale mass casualty incidents using generic triage tools286 and decontamination tents287 can actually cause harm in this population.
Improving geriatric disaster preparedness
Exposure to previous disasters is associated with enhanced resilience, perceived social capital, and optimism among older adults.288
Local leaders can enhance post-disaster social cohesion and trust by promoting the benefits of community preparedness and self-reliance before a disaster occurs, particularly in rural settings.289 Community cohesion is essential, since social isolation after a disaster reduces health-related quality of life.290 Older adults are at increased risk for post-traumatic stress disorder following natural or man-made disasters, but do not appear to be at increased risk for anxiety or mood disorders.291-2
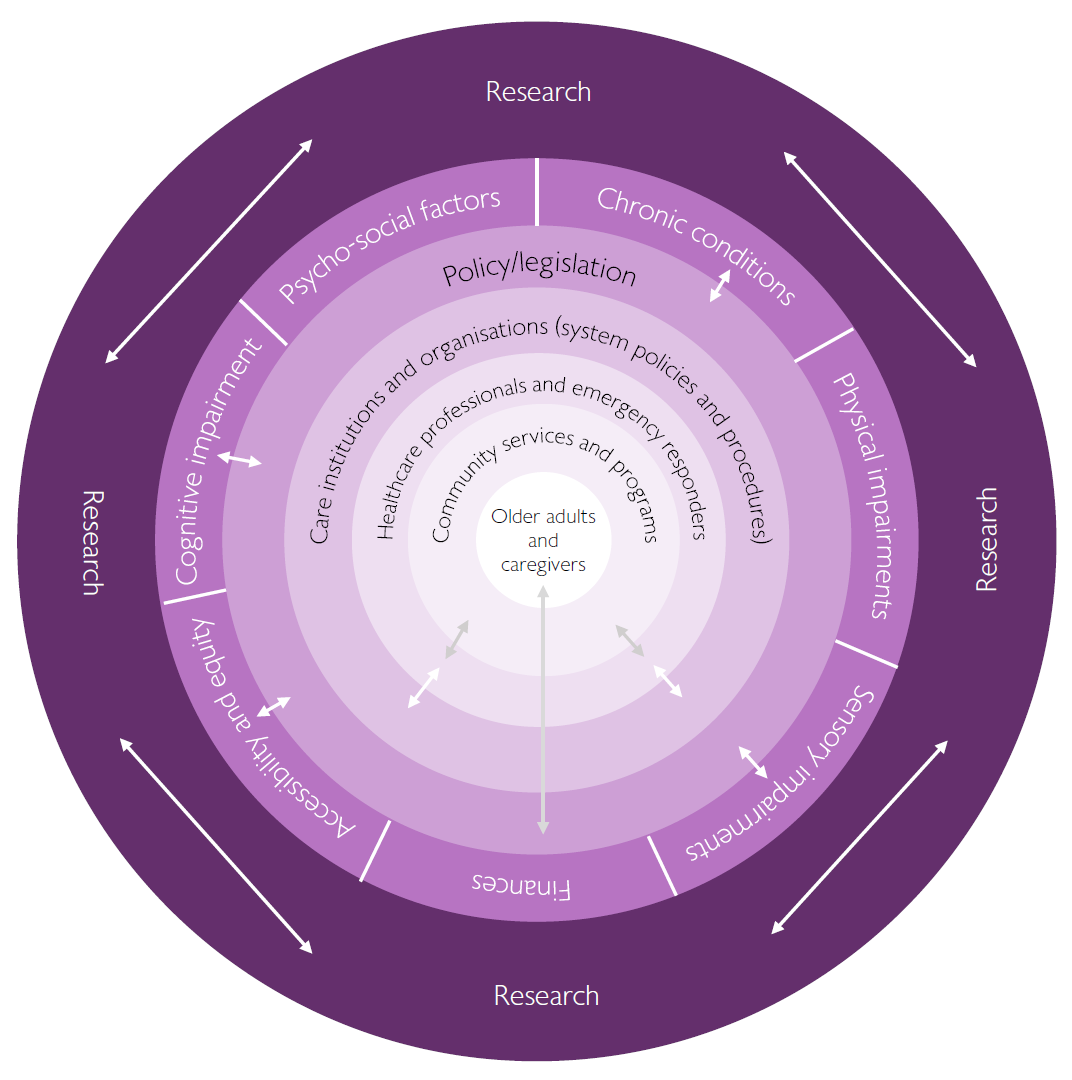
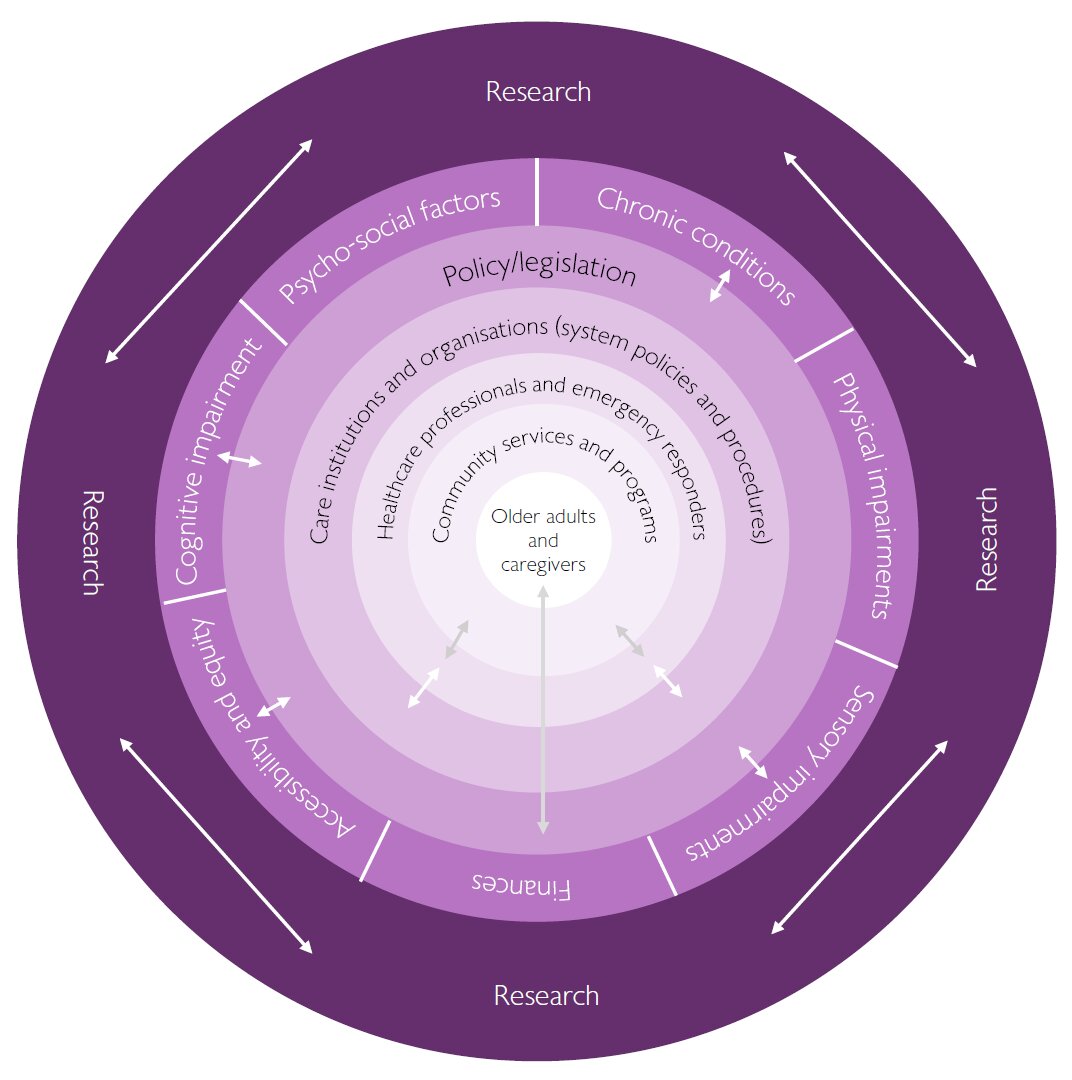
Improving healthcare provider training in disaster medicine principles and geriatric vulnerabilities during catastrophes is essential. Existing geriatric emergency medicine training core competencies and guidelines do not contemplate the unique challenges of disaster care,84,86 and current recommendations on disaster training have limited detail on geriatric care.293 In addition to understanding the negative impact of disasters on older adults and the preventable factors associated with those outcomes, medical providers should be aware all disaster triage schemes among those over age 65 are inaccurate and inadequate for assessing emergent intervention needs, especially in context of those with multiple active prescriptions.286 However, adapting training to incorporate age-specific disaster training is only one component of process improvement. Policy and research advances will be required to sustainably improve older adults’ outcomes during times of disaster (see Figure 6).
Key points
- Preparedness requires pre-disaster engagement of patients, caregivers, local community, and healthcare teams to anticipate barriers to locating, communicating, and transporting older victims, which may require back-up systems for governmental registries and medical documentation.295
- Prioritising research funding that develops frameworks to assess the quality of disaster preparedness across long-term care facilities, hospitals, pharmacies, and other healthcare settings is essential.
- A network of disaster preparedness investigators needs to exist to standardise research methods and efficiently disseminate universal concepts that promote higher quality disaster management for older adults with healthcare crises.
Disasters that impact upon older populations will continue to occur, likely with increasing frequency. Frail older adults are vulnerable to the dietary, environmental, psychological, and social stressors associated with disasters. Advanced planning by families, diverse healthcare providers, and emergency responders will save lives and reduce suffering.

{kind=link}