
Overview
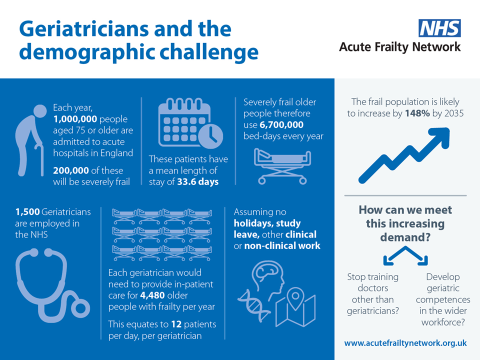
More and more, older people are the major patient group in the context of urgent care scenarios, whether in the acute hospital or in the community. Many older patients living with frailty suffer from a complex combination of multiple diseases, often combining mental, physical and social impairments, yet services are often not designed with these complex needs in mind.
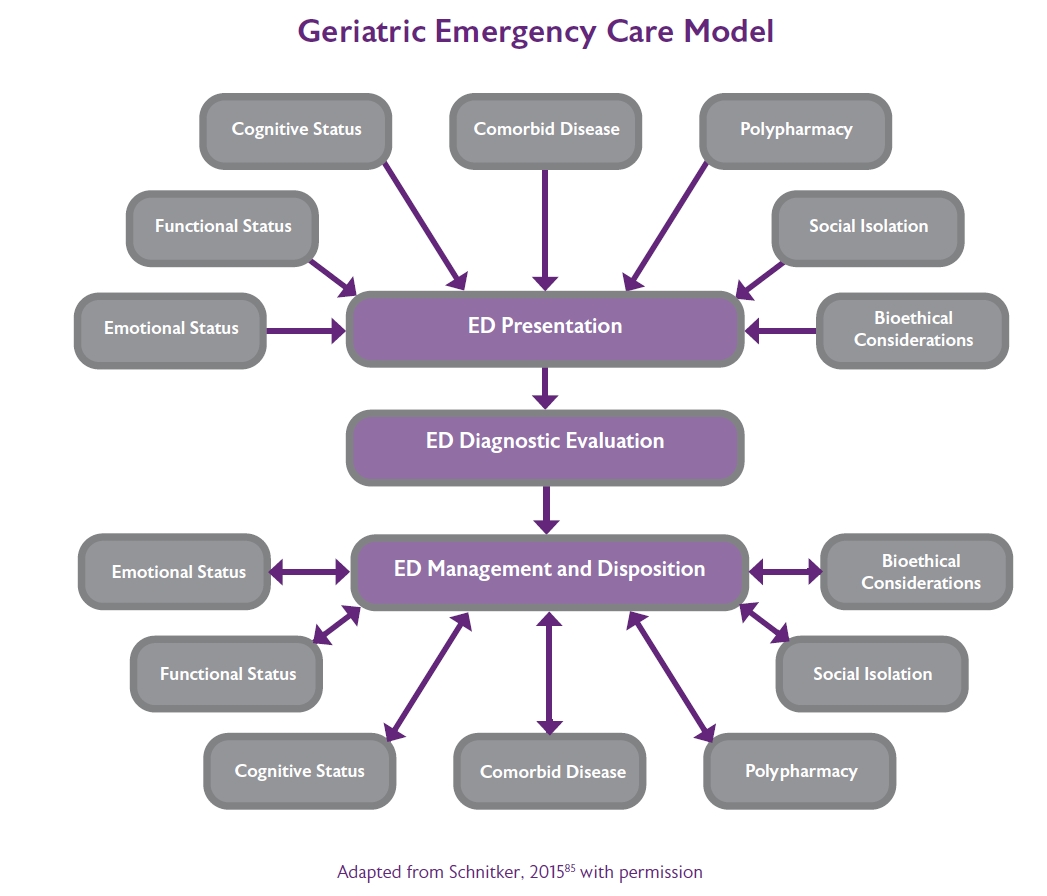
Reaching this goal of high efficiency, while still doing justice to the complexity of the acutely unwell older patient, requires Comprehensive Geriatric Assessment (CGA).44 On the one hand, CGA should identify and analyse specific acute geriatric syndromes (such as delirium), while on the other hand minimise investigations and interventions that do not add value (such as imaging incidentalomas, low specificity biomarkers for pulmonary embolism, acute coronary syndrome, etc). The goal should be to generate a well-informed and well-balanced integrated care decision on whether and how older patients can achieve their prioritised and personalised goals, taking account of prognosis.
Finally, yet importantly, a well-designed CGA approach can make the acute care setting a sustainable and rewarding place to work for a broad range of health care professionals, trainees, and students.
To realise this goal, we need:
- A quick overall review of the complexity of the case (using for example the Clinical Frailty Scale45), taking into account the medical and psychosocial history, vital signs and symptoms
- Shared goal setting fitting the urgency and the stage of life (i.e. aiming for cure or recovery vs. palliative or end of life care
- Determine the approach and interventions that can serve this goal
- Shared decision making to generate a management plan that best fits the individualised personal goal and has the best balance of added value versus risks and burden
- Reflection on action, to assess the benefit, and to learn together as acute care team.
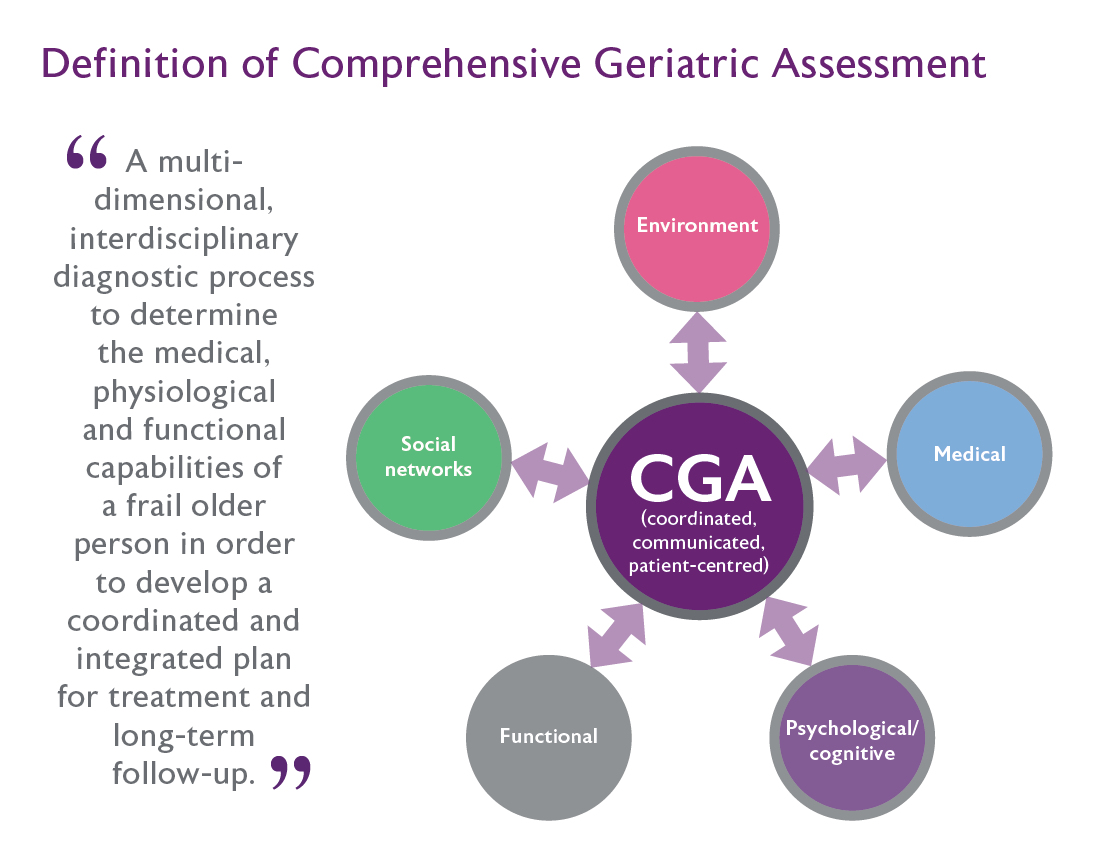
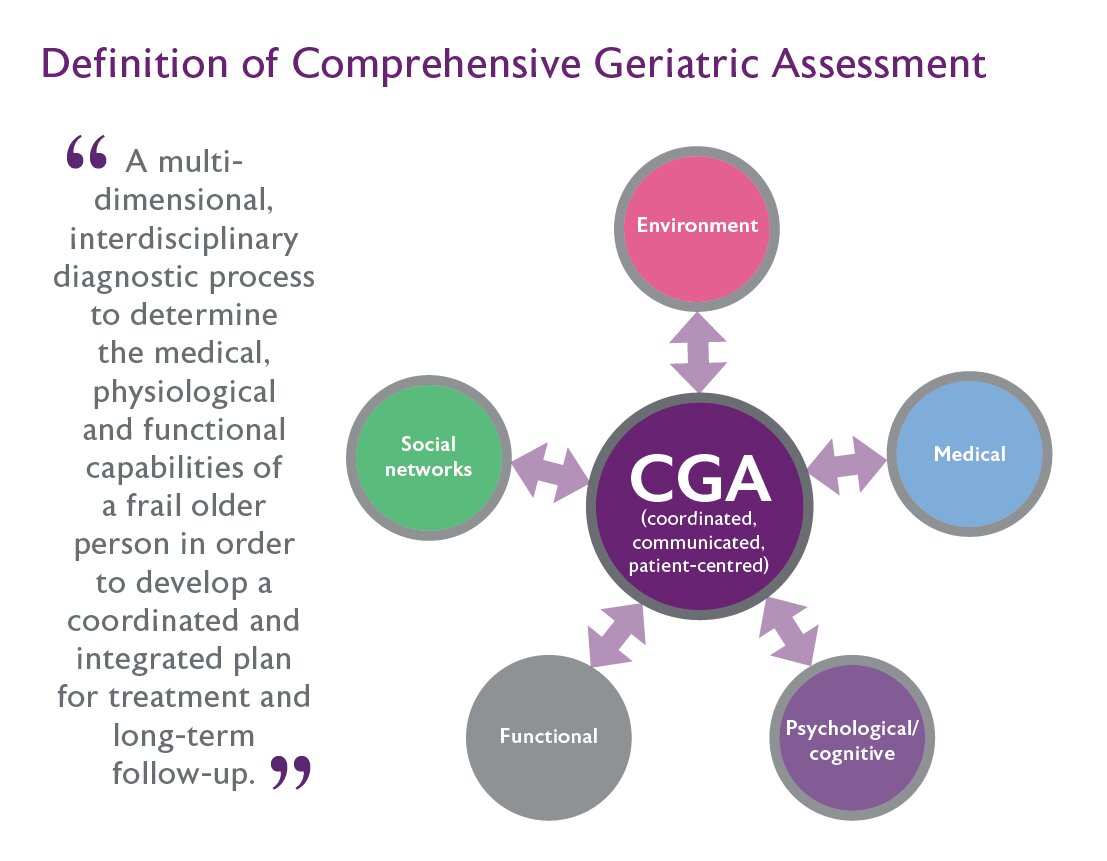
CGA adapted to the urgent care context should combine the core elements of the regular CGA, but with limited time and resources needed, focusing on realising a vital overview, not on secondary details. To reach this, it is appropriate to add the words 'URGENT', 'VITAL' and 'ACUTE' to the widely used definition of CGA - "a multidimensional, multidisciplinary process which identifies URGENT and VITAL medical, social and functional needs, by developing an integrated, co-ordinated ACUTE care plan to meet those needs."
Domains still include medical, functional, physical, mental and social assessments, and information from the caregivers and primary care professionals. This approach should not be short and simple per se. Taking time for an acute care multidisciplinary decision making process involving with the older person and his or her family may still add substantial value, even though it may not seem to fit at the emergency ward. Urgent care settings need to evolve from single problem solutions to add a more holistic assessment of older people with frailty.

{kind=link}
{kind=link}
{kind=link}